Tendonitis: What It Feels Like and How to Start Feeling Better
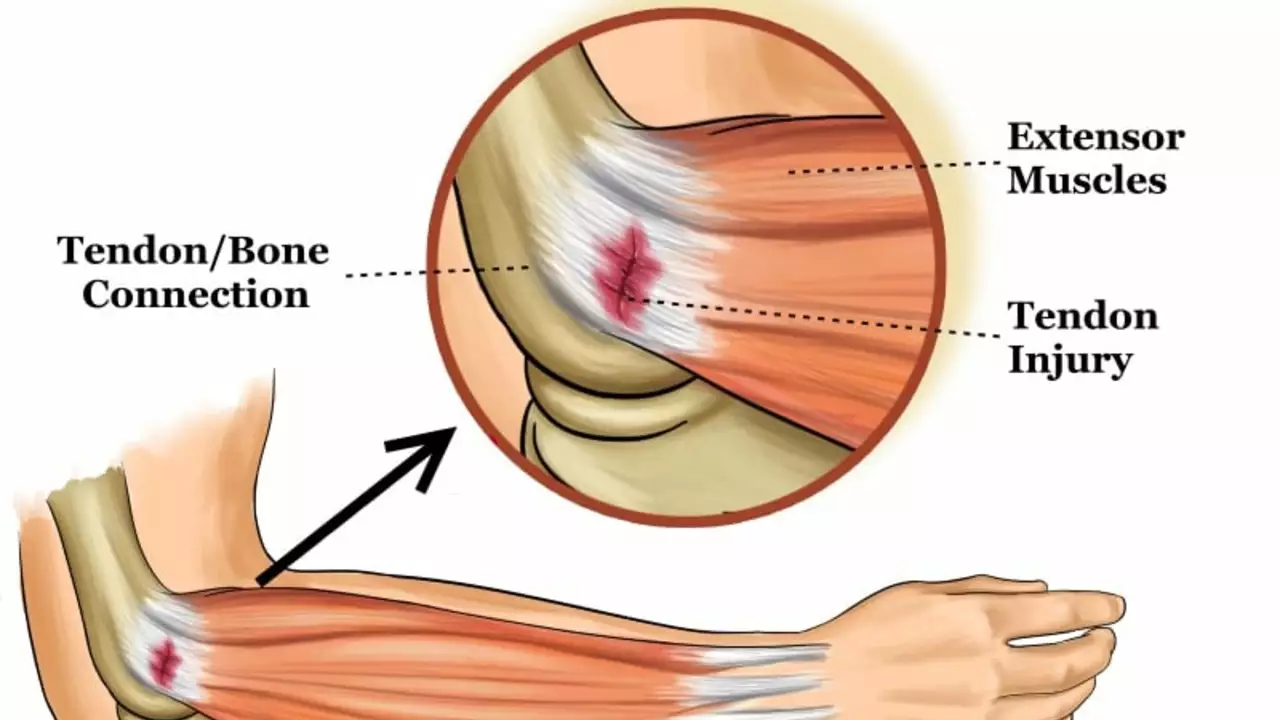
Tendonitis is pain and irritation where a tendon meets a muscle or bone. You’ll often feel a sharp or aching pain near a joint — shoulder, elbow, wrist, knee, or Achilles — especially with movement. It usually happens after overuse, sudden load increases, or poor mechanics. Age and repetitive work make it more likely.
Most cases improve with straightforward steps at home if you act early. The trick is not to rest forever but to reduce harmful load while keeping the tendon moving in a safe way. Below are practical, no-nonsense actions you can use right away.
Simple, immediate steps to ease pain
Stop the activity that caused the pain for a few days or modify how you do it. Apply ice for 10–15 minutes after activity to ease pain. Use over-the-counter NSAIDs like ibuprofen for short periods if you have no contraindications — they lower pain but don’t fix the tendon. A brace or taping can reduce strain, especially for elbow or wrist tendonitis.
If pain is severe, sudden, or you can’t put weight on the limb, see a doctor. Also check in if numbness, tingling, visible deformity, or fever appear. If symptoms don’t improve after 4–6 weeks of focused care, get a medical review — imaging like ultrasound or MRI can check for tears or chronic changes.
Exercises that actually help tendon healing
Eccentric strengthening is the most evidence-backed exercise approach for many types of tendonitis. That means slowly lowering the load on the muscle-tendon unit. For Achilles tendonitis, try heel drops: stand on a step, lift both heels, transfer weight to the painful side, then slowly lower the heel below the step. Start with body weight: 3 sets of 10–15 reps once or twice daily. For tennis elbow, a simple eccentric wrist extension routine with a light dumbbell works similarly.
Begin pain-guided: a bit of discomfort during exercises is okay, but intense pain is a stop sign. Progress load gradually — more reps, then added weight. Pair strengthening with mobility work and posture fixes: tight calves, weak rotator cuff muscles, or poor lifting technique often contribute to tendon stress.
Other options for stubborn cases include physical therapy, guided injections, shockwave therapy, or platelet-rich plasma. Some help, some don’t — discuss risks and expected outcomes with a clinician. Surgery is rare and reserved for persistent tendon rupture or severe degeneration.
Prevention matters: warm up, increase training load slowly, cross-train to avoid repetitive strain, and fix technique issues early. Good shoes, ergonomic work setups, and regular conditioning keep tendons resilient.
Want personalized steps? A short visit with a physiotherapist or primary care provider can set a safe exercise plan and speed recovery. Small, consistent changes beat quick fixes when it comes to tendonitis.